What is unmasking, anyway?
...and is that even the right word for what I'm seeking?
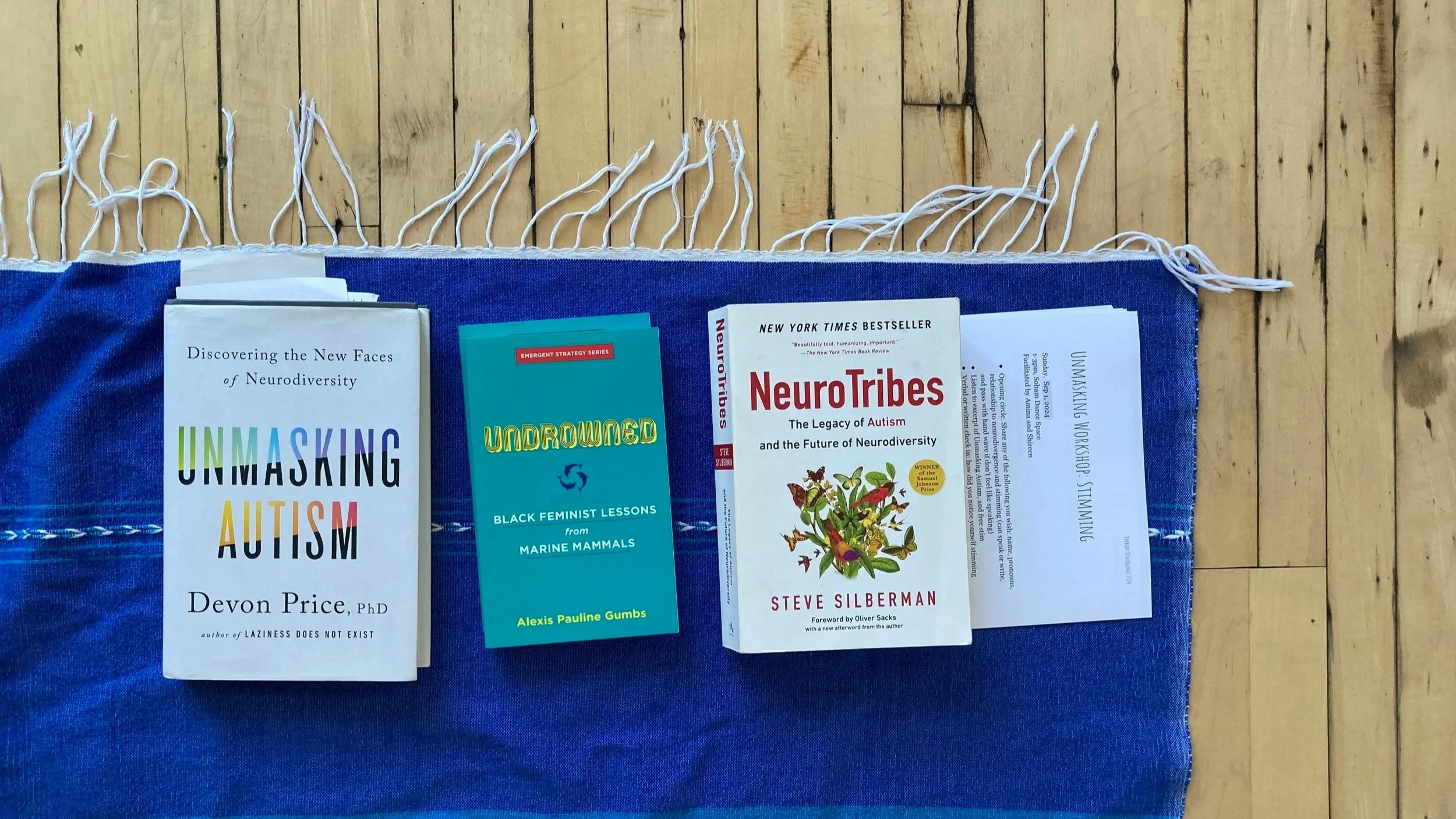
To mask is to perform neuro-normativity—to make eye contact, engage in small talk, and refrain from doing anything “weird” with our bodies. Constant masking without awareness leads to extreme stress and burnout, which has led us to the concept of unmasking. To unmask is the opposite—to release the expectations of our ableist society in order to speak, act, and move freely. It’s a powerful concept, explained in detail by Devon Price in Unmasking Autism.
However, as the concept of unmasking has gained popularity in recent years, it has been used to justify some questionable things. Talking down to others, squashing over other people’s needs to get our own desires met, and ignoring the suffering of people around us in pursuit of constant comfort can all be rationalized as “unmasking.” During a Saturday Night Live appearance in 2021, Elon Musk quipped that he “sometimes say[s] or post[s] strange things,” because “that’s just how [his] brain works” due to his neurodivergence. Given that the things Elon Musk says and posts support white supremacy, it is concerning that he is crediting them to his neurodivergence.
At the British film awards this week, John Davidson, a white man with Tourette’s syndrome, yelled a racial slur at two black actors onstage (Michael B. Jordan and Delroy Lindo). The overwhelming response from white folks was to explain his good intentions and disability rather than to apologize for the harm he caused, as pointed out by black autistic advocate Tiffany "Tiffy" Hammond.
People with power have begun using neurodivergence and unmasking as excuses for doing harm and avoiding accountability.
When we are operating from a place of privilege in this society, we are far too easily positioned to cause harm and call it freedom.
As she did with many things, black feminist poet Audre Lorde warned us about this phenomenon decades ago. In her essay, The Uses of the Erotic: the Erotic as Power, she wrote:
To share the power of each other’s feelings is different from using another’s feelings as we would use a kleenex. When we look the other way from our experience, erotic or otherwise, we use rather than share the feelings of those others who participate in the experience with us. And use without consent of the used is abuse.
Whenever we are with other people, we must attune to them—we must sense for what they are feeling and do our best not to harm them. As humans, we do not exist solely as individuals, and harm to one of us is harm to all of us.
When we “unmask” without sensing for the impact on those around us, we use the feelings of others without their consent.

I don’t want my freedom at the expense of my neighbor’s imprisonment. I don’t want endless resource at the expense of your scarcity. I don’t want to distract myself with constant stimulation or soothe myself with constant comforts while others are suffering. This is not what I mean when I say that I want to unmask.
I want enough for all of us, feet rooted to the ground. I want presence with what is here. I want true liberation, even though that requires me to sometimes feel uncomfortable.
So…is that unmasking? Or is there a better word for it? As I turn this question over in my mind, some terms come to me:
un-severing
re-attuning
un-veiling
de-armoring
re-igniting
I’m not set on any of them yet.
What do you think?
Do you like the term unmasking, or have you found something that resonates more?
Let me know in the comments or by email.
Make it stand out
And if you’re in Chicago, come explore these questions with me in the next monthly Unmasking Lab at House of the Lorde.
Shout out to my partner Blue for teaching me how to discern autism from white masculinity. Blue, thank you for your brilliance, and for talking and living these ideas with me.
“A relaxed body is the most powerful body we have.” -Richard Strozzi-Heckler
I came across this quote by way of Prentiss Hemphill on the We Can do Hard Things podcast.
Such an important reminder this week especially, when I was hit by some sudden losses and shifts.
I’m learning to relax my body when I feel pain, so that it ripples through me and causes me to cry, shake, rock, and wail.
Check your jaw, your shoulders, your hips. Are you clenching to stop something from moving through, or coming out, or hurting you more? Can you let that go?
To handle what’s coming, we need all of us at our most powerful. So, we need all of us at our most relaxed.

Unmasking Workshop
At the unmasking workshop, we gathered, we breathed, we listened, we stimmed...
At the Unmasking workshop last week, we explored 6 qualities of stimming: swaying, clicking, rocking, smacking, swinging, and jiggling.
Can you think of more? What is your favorite way to stim?
At the workshop, we gathered, we breathed, we listened, we stimmed.
I read exerpts of “Unmasking Autism” by Devon Price and “Undrowned: Black Feminist Lessons from MArine Mammals” by Alexis Pauline Gumbs.
People found props like balls and mats to be helpful, and commented on the liberating feeling of being in a room full of other people stimming freely.
If you’d like to be notified about similar events in the future, email me at info@embodydivergence.com and I’ll add you to the Embody Divergence newsletter:)
“Sometimes, I feel like I’m communicating with you underwater.” -Undrowned
Sometimes I feel I am speaking a different language from you, although we both believe we are just speaking English.
Is it because you are a man and I am a woman? Or because I appear less white than you? Maybe it’s because you are autistic and I am not.
My mind tries to compute all the factors at play, but my heart is still racing and my tongue is still stuck.
Over and over, I return to my body. Each time, the path is a little more clear.
In Undrowned: Black Feminist Lessons from Marine Mammals, Alexis Pauline Gumbs writes about the way dolphins use sound both as a way of communicating with each other and as a way of knowing where they are in space. I wonder how much this is true of humans, too. Maybe it is ok to feel like we are communicating underwater. Maybe the sounds we make are sometimes not meant to communicate anything other than “I am here.” Maybe we can still connect with each other, even if we don’t think we understand.
Am I the Villain or the Victim? The Embody Divergence Approach to Social Communication
What if...
Someone perceives something I say or do as racist, sexist, or just plain weird?
A person who is mistreating me is traumatized themselves?
These questions, recently asked by Embody Divergence clients, boil down to: Am I bad, or is it the other person? Whether we deem ourselves or others as "bad," the outcome is usually the same: shame.
In shame, my head hunches, shoulders curl, pulse races, and there's tension in my belly, jaw, and back. Shame leaves me stuck.
The Role of Somatics
Somatics, the practice of body awareness, allows for a shift. By noticing and adjusting my body—inhale, shoulders down, heart open, belly relaxed—I reconnect with myself. Suddenly, I can feel the texture of my socks against my feet. There is more space in my body, and movement feels possible.
At Embody Divergence, we…
Move beyond the good/bad binary, deconstructing ableism and all isms
Sense our inherent potential for growth, curiosity, and love, despite systemic and personal traumas
Soften into authentic expression and connection with others
In sessions, clients are guided through conversation, prompts, and movement. This isn't traditional speech therapy. Instead, it challenges the binary of good and bad, drawing from de-colonial and indigenous traditions to ask: What if there's nothing wrong with me? What does that free in me, and how does it allow me to show up in the world?
This is our current journey at Embody Divergence. Join us, forward this message to those who might benefit, and explore our offerings.
Offerings
There are two free Embody Divergence classes coming up this summer: Somatics for Neurodivergent Folks, and Cross-neurotype Communication for Siblings. Find out more and reserve your space here.
Embody Divergence is growing! Speech therapy, somatic facilitation, and business consulting spots are available. Book a consult here.
Curiosities? Commentaries? Email info@embodydivergence.com
The Learning Wound
Many of us have a learning wound– a way in which the naturally joyful process of learning has been twisted to become something unpleasant and scary.
When I was a kid, I loved learning. I would spend hours reading a book or learning a new skill, completely present in the process, in a flow state. Around my early teen years something shifted: I started to notice something in the tone of a teacher’s voice or in the glances of other students that made my chest and throat tighten, and my pulse quicken. Thoughts like “I should be getting this faster” and “why can’t I remember anything?” swirled around in my head and made it harder and harder for me to concentrate.
From a nervous system perspective, the learning wound arises when a person is pressured to perform when they do not feel safe. True learning is a form of play, and play happens in the parasympathetic state, when a person feels safe and connected to others. Play cannot happen when a person feels that they are not safe and accepted.
Much of my work with myself and with my clients lately has been around tending to this wound. Can we grieve the ways we have been forced to perform while not feeling safe, and the deep disconnections that has created? Can we cultivate enough grounding and safety so that we can start to learn again, from a place that feels genuine and juicy? Can we remember that actually, we love learning?
Does this resonate with you? Do you have a learning wound? When did it first start to appear? Can you remember what learning felt like in your body before you were wounded in this way?

Frequency Matching
While working in a clinic with autistic kids, I learned something crucial about healing work. If a child was having a meltdown and I went to them and said “calm down” in a calm therapist voice, it did not work. Usually, this would make the kid even more upset, which would make me upset too. But if I went to the kid and matched them where they were at, something different happened. For example, if they were sitting on the floor yelling “no no no,” then I would sit on the floor and yell “no no no” with them. When I did this, something clicked, and often the child would start to emerge from the stuck place they were in.
This is how I approach so much now–whether it's songwriting, a difficult conversation, or working with a client. I start from the frequency of where we are. I be with that, with my whole self. And then I wait, and things start to shift on their own. I don’t force anything, and it feels like magic.
A sore tailbone and the way being watched changes the essence of the thing.
When I arrived at the jumping place in San Marcos for the first time, I was centered. As I stepped off of the platform with my heart racing, I said to myself “I surrender” and I fell down, down, down, toes pointed, body relaxed, and slipped easefully into the water, 30 feet below. I emerged, laughing, “that was fun!”
Yesterday as I walked to the jumping place in San Marcos, I noticed that I didn’t really feel like jumping. But when I arrived, a handsome man was there. “Si tu saltas, yo salto,” he purred at me, and my heart began to race again, but this time with a different quality to it–thumping out of my body and filling me with a sense of urgency. I ran off of the platform, arching my back in a centerless desire to be seen by him. Time and space blurred. THWACK. My body hit the water flat like a pancake, sending a stinging shock through my whole being. There was a collective groan of empathy from all the onlookers, including the handsome man, who proceeded to do an elegant backflip into the water and never speak to me again.
After a good cry and a hug from my friend, I was able to laugh, and to notice: How drastically my movements shifted out of integrity when I was performing for this man’s gaze! It reminded me of a physics experiment I read about in which scientists looked at how light particles move when observed versus unobserved, and found that the presence of an observer changes the quality of the movement. It also reminded me of something I see often in my work: when we are trying to perform for a gaze–things go wrong. People who stutter often don’t have much difficulty speaking when they are in a speech therapy session, because fluency does not feel required in that space. People with social anxiety feel fine about expressing themselves when it’s to somebody they trust.
Today, my tailbone is sore, and I am grateful for the reminder: Amina, move with integrity.


Liberation
“If you have come here to help me, you are wasting our time. But if you have come because your liberation is bound up with mine, then let us work together.” – Lila Watson
“If you have come here to help me, you are wasting our time. But if you have come because your liberation is bound up with mine, then let us work together.” – Lila Watson
In the last 2 years, I completed my master’s degree in Speech Language Pathology. While my master’s program was incredibly rigorous and taught me many important things about speech and language, I found myself noticing by the end of it that we had failed to learn the most important thing of all: that being a clinician is as much about helping yourself as it is about helping others. Perhaps this is something that an academic program can’t really teach, and so I’m grateful to the life experience that has brought me to this awareness as I begin my first year as a Speech Language Pathologist (SLP). By telling a piece of my personal story here, I hope to illuminate for fellow SLPs, clients and their family members, and anyone interested in communication in general what I mean when I say that my liberation is bound up with the liberation of the people I work to help.
I remember the first time I heard my brother’s label: autism. I was 8 years old, on my way to piano practice when my mom told me. Before that, I had just thought of him as my brother. Eccentric for sure--he loved to talk about history and draw dinosaurs. But then again, I was eccentric too--I liked to do my homework in a closet while dancing to the Spice Girls. Once I knew that he had that label though, it changed how I related to him. In some ways it helped, because I could now realize that sometimes when he was annoying me it was just because he was experiencing things differently. It also helped him to get access to resources he needed like therapy and extra time on tests. Often though, the label made it harder for me to relate to him, because I was so conscious of there being something “wrong” or different about him. I became so concerned that he would do something weird in front of other people that I would always make sure to let people know that he had autism before I introduced him to them. I became so worried that someone else would make fun of him for how he talked or acted that I spent the majority of my time with him correcting him: telling him to fix his hair, stop scraping his fork against his plate so loudly, and stop talking so much about history because nobody was interested. As a result, my brother became more closed off towards me, and I started to feel guilty whenever I thought of him.
I carried this guilt pretty heavily, and it occupied my conscience so much that it led me to pursue an unusual path: the career of Speech Language Pathologist. I thought that if I could understand what was wrong with my brother and help other people like him, then I could help him, help my family, and ultimately help myself. What I didn’t know then was that my logic was backwards: I needed to understand myself better first, not my brother.
As you read this, I invite you to think of a situation in which you have felt such a strong sense of guilt or judgement towards someone that it made you feel uncomfortable whenever you thought of them. Keep that experience in mind as I tell the rest of this story, and maybe it will lead you to a similar realization as the one I am about to describe here.
Over the course of my time in my master’s program, a few pivotal things happened in my life that had nothing to do with grad school. My family went through a big conflict, and in a dramatic display of anger, I shaved my head. Then, the COVID19 pandemic hit. Suddenly, I was isolated in a house with my mother, my father, my brother, and all of our issues, and I had a haircut that made me look like a 9 year old boy. It was an interesting time, to say the least.
With so much time alone, I began to unravel layers of myself. I stopped wearing makeup, and started wearing my ex-boyfriend’s clothes. Without much contact with the outside world, I started to realize that there were many aspects of my identity that I thought were me, but were really just things I had been told were me.
The past year has been a delicate process of unfurling, as I have emerged from this place of deep introspection. I realized that how I communicate with others is a direct reflection of how I speak to myself in my head. When I tell my brother that nobody will like him if he looks or acts a certain way, I am telling myself that I am not worthy of love if I don’t look or act a certain way. What a painful thing that is for both of us to hear.
As I begin my career as an SLP, I run into this same dynamic frequently. The family members of people with communication challenges often criticize that person at home in an effort to shield them from criticism out in the world, without realizing that their words cause just as much harm as a stranger’s. And not only does it harm the person they are speaking to, it harms the person who is speaking too. So how do we escape this well-intentioned but harmful pattern of communication?
This question brings me back to the Lila Watson quote about liberation that I began with. In order to help others, I have to begin with myself. I am making it a part of my practice as an SLP to ask myself questions like:
What can people with autism teach me about social norms?
What can people with ADHD teach me about attention?
What can people who stutter teach me about speech?
One of my clients who stutters told me the other day that he is hyper-aware of his flaws and tries to hide them at all costs, whether it’s his stutter, or a mole he doesn’t like on his face. He told me a story about a classroom of kids and teachers staring at him with confusion and judgment as he struggled to get a word out in response to his teacher’s question. Moments like that are part of what causes him to hide his stutter to this day. It sparked the memory for me of a boy in my kindergarten class telling me I had “man arms.” It was such an insignificant comment, so long ago, and yet I have been removing the hair from my arms ever since. I told my client this, and while neither of us had a resolution to offer, I felt something click between us.
The more I learn, the more I see that the clients I work with teach me just as much as I teach them. As I’ve become gentler towards myself, I’ve noticed myself soften towards others as well. I no longer have the urge to judge or correct my brother all the time, and when I do, I am more able to pause and reflect on the impact of my words before I say them out loud. This shift has led to something beautiful, which is that I can finally relax and enjoy hanging out with my brother again, instead of always trying to change him. This past summer, we went on a walk to the beach together where he encountered a hermit crab. I listened to my brother as he carried out a 5 minute conversation with this crab, who he named Martin. The creativity and wit of this very one-sided conversation made me laugh so hard that I cried. My brother laughed too and patted me on the head, “I’m glad you’re here Meanie,” he said. I was glad too. I had missed my brother so much.

Empathy: the most important clinical tool
Empathy is the most important clinical tool
There is no such thing as a communication disorder; there are only people trying to communicate. There is no such thing as speech and language pathology, just the pathologization of language practices." -- Betty Yu
As a clinical fellow, I have regular supervisory meetings to discuss my caseload and work through any challenges I’m having. In one of my meetings with my supervisor recently, I shared two cases with her in which I was feeling stuck. The way she responded to these scenarios illuminated something very important that I hadn’t acknowledged before: when working as a speech therapist. empathy is an essential clinical tool.
While it may seem obvious to approach clients with empathy, I hadn’t thought of empathy before as an actual tool to inform the evaluation and treatment process. Here is how this concept became clear to me.
The first case I shared with my supervisor was that of a teen with a nonverbal learning disability and slow auditory processing, who does not engage much with others socially. There are long periods of silence between when I ask a question and when they answer, and they only respond in one-to-three word utterances most of the time. They are able to produce longer utterances, and grasp fairly complex concepts, but most of the time, they don't. Their parents are concerned, because this teen spends a lot of time alone and doesn't have close friendships. I had reached a standstill with this client because I kept introducing topics and questions to them and being met with a minimal response.
When I described this situation to my supervisor, she thought for a moment. “Well,” she said, “If it took me a long time to process auditory information, I would probably not want to ask a lot of questions, because I would know that then I would have to listen to the response.”
She suggested that instead of conducting our sessions as verbal conversations, I could incorporate visuals that we could look at together, and give the client the option of using the chat feature instead of talking.
The second case I shared with my supervisor was that of a client who was born without hearing, and who had a hearing device implanted as a toddler. This client’s speech is currently about 60% intelligible to an unfamiliar listener due to their way of articulating sounds. This client’s way of speaking was unlike anything I had heard before, and I was having trouble understanding the ways that they were producing speech sounds. My supervisor asked me to consider the question, “What would it feel like to make speech sounds if you couldn’t hear yourself? Where would you feel the sounds in your mouth and throat?” After I considered this, she shared with me that often, people with hearing loss make sounds further back in the throat because they can feel the vibrations of them more strongly there than they can when the sound is being made further up towards the front of the oral cavity. Because of this, part of my work with this client would be teaching them to deepen their tactile awareness of how sounds feel when they are produced further forward in the oral cavity.
In both of these instances, my supervisor used empathy in order to understand what was impacting the client’s method of communication, and how to proceed with treatment. This lesson has greatly impacted the way I approach my clients, and it led me to create the following empathy-based process for how to approach my work:
Step 1: Gather information about the person. Do any relevant formal or informal testing, and find out relevant details about their physical, mental, and emotional history. Find answers to questions like: How do they currently communicate? What is their day to day environment like? What demands are being placed on them by work, school, and community? What diagnoses do they have? What interactions with the medical system have they had?
Step 2: Do your research. Learn whatever you can about the diagnoses and conditions that they have, and the meaning of their test results. This is the part that graduate school prepared you for, so nerd out with confidence!
Step 3: Empathize. Given all the information you have collected about the person, imagine that you are them. Let yourself sit in that space, without rushing to come up with any answers. Once you have settled in, start to ask yourself questions like: How would I spend my time? What would I want to avoid? What might I believe is bad or shameful about me? How might I hide or try to compensate for things that I’ve been told are wrong about me? How might I advocate for myself? What are my needs? How would I seek to get my needs met?
We can never truly know what it is like to be another person, but by doing our best to empathize with our clients, we can treat them as human beings who are trying to communicate, rather than as something to pathologize.